28Sep, 2023
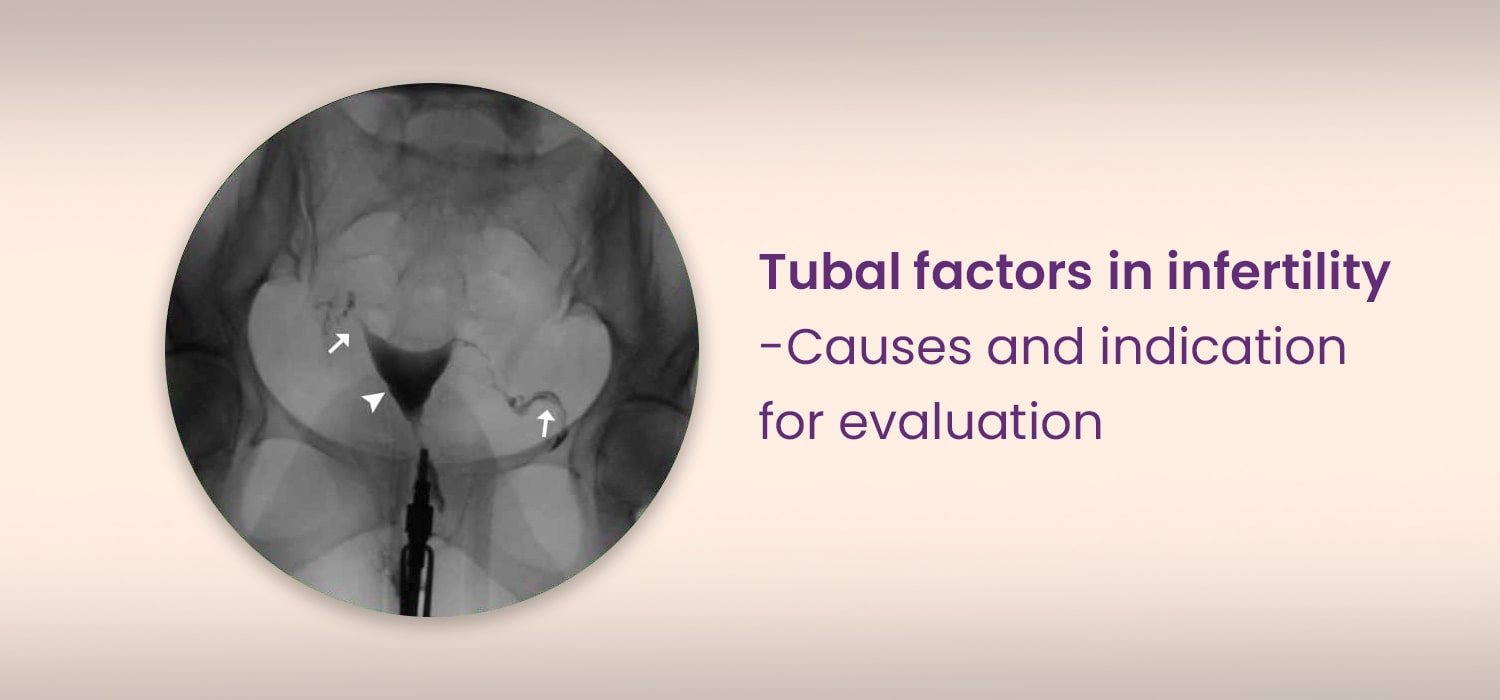
Tubal factors in infertility-Causes and indication for evaluation
Tubal factors account for 25-35% of female factor infertility.
The causes of tubal subfertility are always due to acquired factors. These include proximal/ mid or distal tubal disease which is often due to pelvic inflammation. Congenital tubal factors causing subfertility are rare.
Proximal and mid-tubal disease
This accounts for 10-20% of tubal disease.
Proximal obstruction can be a pseudo-obstruction due to plugs of mucus or amorphous debris, cornual spasm, viscous secretions, and mucosal agglutination. True obstruction occurs in Salpingitis Isthmica Nodosa (SIN), Pelvic Inflammatory Disease (PID), Endometriosis, Cornual Polyps and Intra-Uterine Synechiae.
Mid-tubal obstruction results from PID, endometriosis, post-surgical inflammation and adhesions causing stenosis and occlusion, bulbous termination, scarring and fibrosis.
SIN is tubal inflammation of unspecified origin, affecting the proximal tube. There could be involvement of the distal part of the tube also associated with pelvic adhesions and adhesions in the peri-hepatic areas ( Fitz-Hugh-Curtis syndrome). Histopathology in SIN reveals myo-salpingeal hypertrophy with endo-salpingeal diverticulae.
PID and endometriosis can cause tubal occlusion by direct involvement or secondary to adhesions.
Distal tubal disease
Accounts for 85% of tubal infertility. PID is the main cause . 85% of PID is due to sexually transmitted diseases viz-Gonococcal, Chlamydial and Mycoplasmal infection. Tuberculosis-especially in countries like India- is another chief cause. Peritonitis due to any cause, previous surgeries and endometriosis are other causes of distal tubal disease.
Evaluation of tubal factor infertility
Evaluation for tubal factors is indicated when history and ultrasound indicate high suspicion of tubal disease. This includes history of PID, endometriosis, previous pelvic surgery, or ectopic pregnancy. Tests for tubal factor infertility is also indicated, even when there is no suggestive history, when the couple fail to conceive even after 3 months of treatment with ovulation induction with timed intercourse or IUI (Intra uterine Insemination)
Societal Guidelines for testing of tubal factors for infertility
- RCOG-The recommendation for suspected tubal/ uterine factors include:
- When there is no suspicion of PID, previous endometriosis or ectopic pregnancy, HSG for screening of tubal occlusion can be offered. Alternatively, HyCoSy ( Hystero-salpingo contrast sonogram) can be done, if available.
- In the presence of suspected co-morbids, laparoscopy with chromopertubation can be offered.
- Hysteroscopy must not be offered as the initial part of the investigation unless clinically indicated.
- ESHRE (2000)
The three categories of testing for the couple. which were found to be associated with a healthy pregnancy outcome were Semen, analysis, tubal patency tests ( Hysterosalpingography or Laparoscopy) and ovulation testing. The 2008 guideline specifies that the first line of investigations, namely Semen analysis and Ovulation assessment ought to be followed by laparoscopy if there exist associated co-morbidities. - ASRM
ASRM recommends that tubal disease must be ruled out by doing tubal patency tests and Chlamydia antibody testing.
HSG, SIS ( Saline infusion sonography), laparoscopy with chromopertubation, selective canalization of tubes by fluoroscopy or hysteroscopy are proposed as being complementary and not mutually exclusive methods of tubal patency testing. More than one method is required for testing.
For more info, Visit : www.medlineacademics.com